

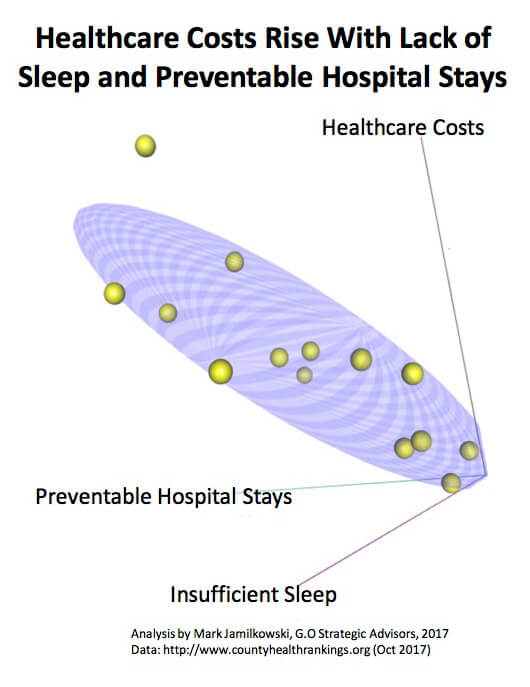
Elliptical region represents the projected region of correlation, ie the zone where all relationships between cost, preventable stays, and insufficient sleep would likely be. The graphi indicates positive correlation or positive relationship between preventable hospital stays, insufficient sleep, and healthcare costs (ie as preventable stays increase and/or insufficient sleep increases, healthcare costs increase as well.)
Healthcare-based treatment and therapeutic applications of Virtual Reality (VR) are emerging at a rapid pace, impacting patients, physicians and health insurers as well. VR applications such as Mindmaze target recovery from trauma, strokes and head injuries, and still others like Firsthand Technology or appliedVR look to reduce or treat pain. Recently I was inspired and moved by a published testimony given by a chronic-pain patient suffering from Lupus who received near-immediate benefit from an app running in a VR HMD (Head Mounted Display). This is also remarkable for the unintended socio-economic impact; the controlled distraction and subsequent relief from pain that immersive VR activity can provide has the potential to also address another healthcare crisis receiving headlines recently, namely over-use and misuse of prescriptions and addictive use of opioids. Other quality-of-life based applications target mental and physical well-being. These innovations have significant implications for health insurance plan design and cost.

MindMotion™ PRO is FDA-cleared to bring 3D virtual environment therapy for neurorehabilitation to patients in the United States. SOURCE: Mindmaze
There have been numerous studies published by the AHA, the National Institutes of Health and psychiatry publications including PsychCentral that have identified increased mental and physical stimulation as reducing risk of hospitalization and potential readmission. In 2015, The International Journal of Diabetes published an article “Physical activity reduces the risk for hospitalizations in patients with type 2 diabetes.” Separately, an analysis was done for this article examining drivers of health insurance costs using a range of metrics, including clinical, demographic, socio-economic, environmental and quality of life. The was a notable correlation between activity, hospitalizations, and cost of health insurance for the counties analyzed, representing a sample across the United States representing large cities as well as small, with varying levels of economic circumstances. This analysis confirmed a high correlation between increased healthcare insurance costs and drivers such as obesity and diabetes, and statistics related to preventable hospitalizations. Incidence of obesity and diabetes were also strongly correlated to metrics tracking diet, exercise and personal behaviors.
Behaviors such as drinking alcohol and smoking were found to be highly correlated with tracked stress-related indexes. But stress isn’t necessarily caused exclusively by behavior. For these indexes, the root cause of stress can be summarized into two components. Stress may come from societal factors that need to be addressed through public policy, such as crime, youth-based employment, child poverty, and single-parent homes. Part of the source of stress is being collected in social determinant information such as income, living conditions, and access to a reliable source of food. This latter set of conditions are in bounds for care management protocols, and VR-related applications, if the industry is truly moving to community-based care and population health-minded protocols.
The use of VR like VirZoom, GestureTek, and OmniVR are looking to revolutionize physical engagement of the patient, and physical activity has been proven to directly and favorably impact overall sense of health and wellbeing, as well as expected rates of initial hospitalizations and recovery times. This has significant implications for cost savings and required changes to care management protocols. A 7-10 percentage point improvement in people reporting being physically active has the potential to reduce healthcare costs by 15-20% based on this analysis. VR is following in the footsteps of the impact tele-health based applications have had. Tele-health based initiatives have already shown tremendous favorable-cost impact through greater interaction and in lower cost settings, expanding access and reducing cost at the same time.
There are obstacles to realizing these savings and changes to care protocols. Insurers are likely to characterize a VR-based treatment as experimental for now. The full reasoning (and clinically-tested proof) behind the effectiveness of VR technology is still emerging. Academic articles, such as those published by HHS, look beyond the controlled distraction aspect of VR and explore the internal psychological and biochemical responses that augment the technology-based environment. The question of “how it works” becomes critical if Chief Medical Officers are to determine how best to coordinate the care with other parts of the care delivery continuum. Additionally, insurers face the challenge of integrating data from various platforms, including claims data, clinical/EHR data, and information from VR, tele-health or other forms of patient interaction. Operationally, this data must be interwoven into the care management policies and protocols shared between physician and health plan. This will require substantial effort and resources, given historical legacy platforms and systems.
Opportunities to apply VR solutions appears to be significant, creating better care delivery, improved quality of life, and cost savings across the system. VR applications hold promise to significantly change the care management processes insurers use, and can be another data point in population health based care management and patient engagement, but the technology by itself is not enough; it must be coordinated with other aspects of the system. This article doesn’t address operational and enterprise-level non-treatment use of VR within health care systems, which may add, most ironically, additional pressure and stressors for insurers and the non-clinical workforce.
Barriers to VR adoption, such as bulkiness and cost, are quickly being addressed by innovators; cost alone is a third of what it was 5 years ago. I see the remaining major hurdles to widespread and rapid increase to using the technology within the next 5 years are the challenges health plans face. I suggest they consider VR treatment-specific applications a prescription versus durable medical equipment in benefit plan designs, and work with network physicians to provide the right incentives to realize the savings implied above. VR innovators would be well positioned to help insurers address this nightmarish challenge by partnering with data aggregation innovators and participating in the design of a common data platform. The next five years will tell the tale of those who will be gone, those who will have transformed themselves to thrive, and new entities that couldn’t have existed before without the new technology, not only amongst the VR innovators but the insurance providers as well.










